WHAT IS IT?
The ulnar collateral ligament (UCL) complex connects the humerus (upper arm) to the ulna (forearm). The complex is composed of three ligaments: the anterior band, the band, and the transverse band. They act to stabilize the elbow during certain motions such as throwing, with the anterior band being the most important. UCL tears occur most commonly in athletes who participate in repetitive overhead sports, such as baseball and the javelin throw.
WHAT ARE SIGNS AND SYMPTOMS OF A UCL TEAR?
Common symptoms of UCL Tears include:
• Pain along the inside elbow when throwing
• Decreased velocity
• Loss of control when throwing
• Numbness and tingling in the ring and little finger
DIAGNOSIS
In the office, a complete history and physical exam is obtained. Careful measurements of range of motion and strength are recorded. Special testing of the UCL can help elicit the symptoms experienced during throwing. Oftentimes, diagnostic imaging, such as X-rays and MRI, are necessary to confirm the diagnosis.
Conservative treatment of UCL tears is generally recommended in partial tears. Such treatments include rest, ice, anti-inflammatories, and physical therapy. Cessation of throwing is recommended for at least six weeks. Biologic treatments, such as platelet rich plasma (PRP), can help improve healing.
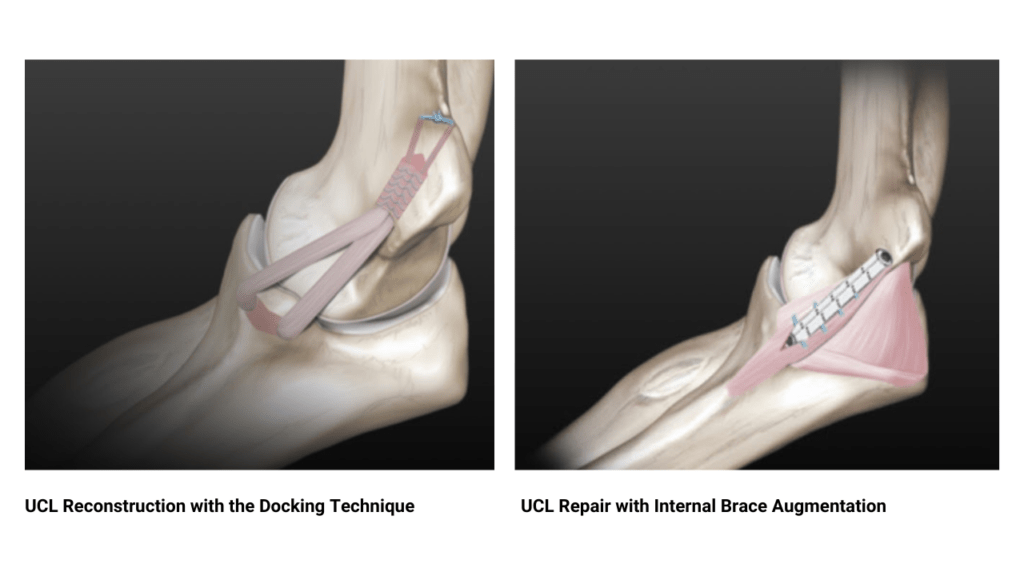
Surgical treatment of UCL tears is recommended in patients where nonsurgical treatment has failed but wish to continue with overhead athletics. UCL reconstruction (Tommy John Surgery) consists of rebuilding the UCL complex by creating tunnels in the bone and passing a graft through them. The two most common UCL graft choices are the palmaris tendon in the forearm and the gracilis hamstring tendon.
In rare circumstances, the torn UCL is healthy enough to repair. This scenario is most common in younger patients, where the ligament has not experienced significant wear and tear. In these cases, UCL repair involves securing the torn tendon to the bone with small suture anchors.
TREATMENT
Patient setting under regional anesthesia, allowing patients to return home the same day. In conjunction with supervised physical therapy and a structured throwing program, UCL reconstruction has been shown to successfully return patients to throwing.
RECOVERY
Following surgery, patients are placed in a splint for one week and then transitioned into a brace for six weeks. Physical therapy begins early with emphasis on range of motion. Strengthening begins around three months, followed by a throwing program at four months. Patients generally return to competitive throwing at 12-18 months postoperatively.