What is it?
The medial collateral ligament (MCL) is a stout ligament on the inside aspect of the knee that connects the femur (thighbone) to the tibia (shinbone). Its primary function is to prevent the knee from bending inward (valgus). Injuries to the MCL occur when the knee is struck from the outside. It is commonly seen in contact sports such as football, soccer, or basketball.
WHAT ARE SIGNS AND SYMPTOMS OF AN MCL INJURY?
Common symptoms of MCL tears include:
• Pain along the inside of the knee
• An audible pop
• Pain and swelling
• Difficulty walking
Diagnosis
In the office, a complete history and physical exam is obtained. The knee is examined for any deformity or tenderness to palpation. A comprehensive test of all the ligaments is performed and oftentimes compared to the uninjured side. Imaging studies, such as an X-Ray and MRI, may be necessary to confirm the diagnosis and identify associated injuries, such as an ACL tear.
Treatment
The vast majority of MCL tears can be treated with conservative management. Such treatments include rest, ice, anti-inflammatories, and physical therapy. Crutches and a knee brace may be used initially to support the injured knee.
Surgical treatment of MCL injuries is generally recommended in active individuals who failed nonoperative treatment or have multiple ligament injuries in the knee. MCL repair is performed by reattaching the torn ligament back to the bone. In chronic situations, a free graft may be necessary to augment ligament (MCL reconstruction). These procedures are typically done in an outpatient setting under regional anesthesia, allowing patients to return home the same day. In conjunction with supervised physical therapy, MCL surgery has been shown to successfully return patients to their sport or activity.
RECOVERY
Following surgery, patients are placed in a long hinged knee brace for six weeks. Physical therapy begins within the first week of surgery, with emphasis on knee range of motion. At six weeks, the brace is removed and the focus turns to gait training and strengthening. A jogging program is initiated about 3-4 months postoperatively, followed by an agility program at 5-6 months. Sport specific drills are initiated at six months, and patients generally return to sports around 9-12 months postoperatively.
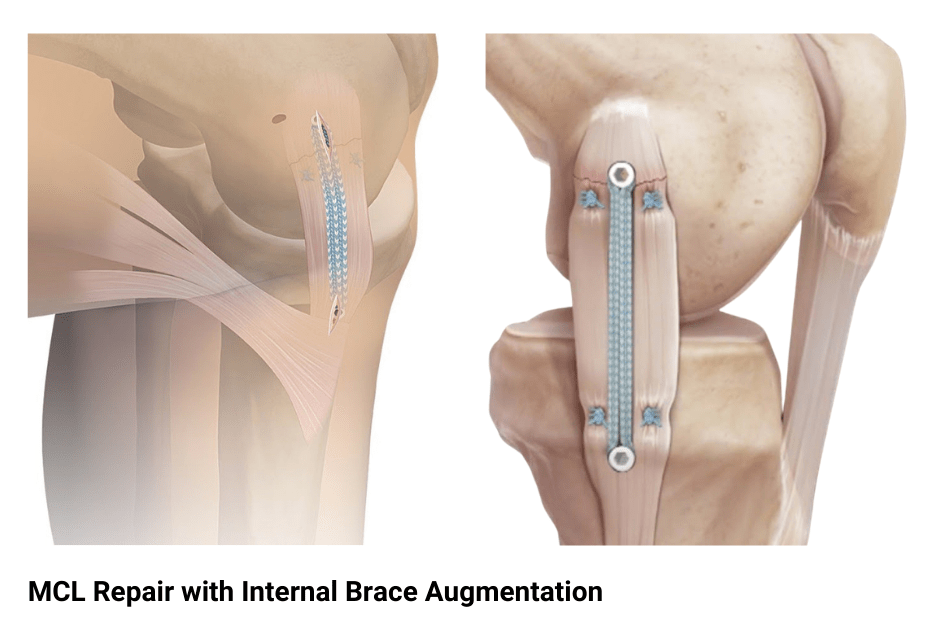
MCL Repair Animation
This animation demonstrates augmentation of an MCL repair with an internal brace. Following an MCL repair, an anchor loaded with a broad suture is inserted into the femur. A point on the tibia is then identified to be the isometric point, where the anticipated suture does not lengthen or shorten with knee range of motion. At this location, the second anchor is placed with the suture appropriately tensioned and thus augmenting the MCL repair.