Conservative management of patellar tendon injuries can be performed in partial or incomplete tears. Accurate diagnosis is essential, as many patellar tendon injuries are complete ruptures. Patients are first braced with the knee in extension for six weeks. Range of motion is then gradually permitted following this period of immobilization.
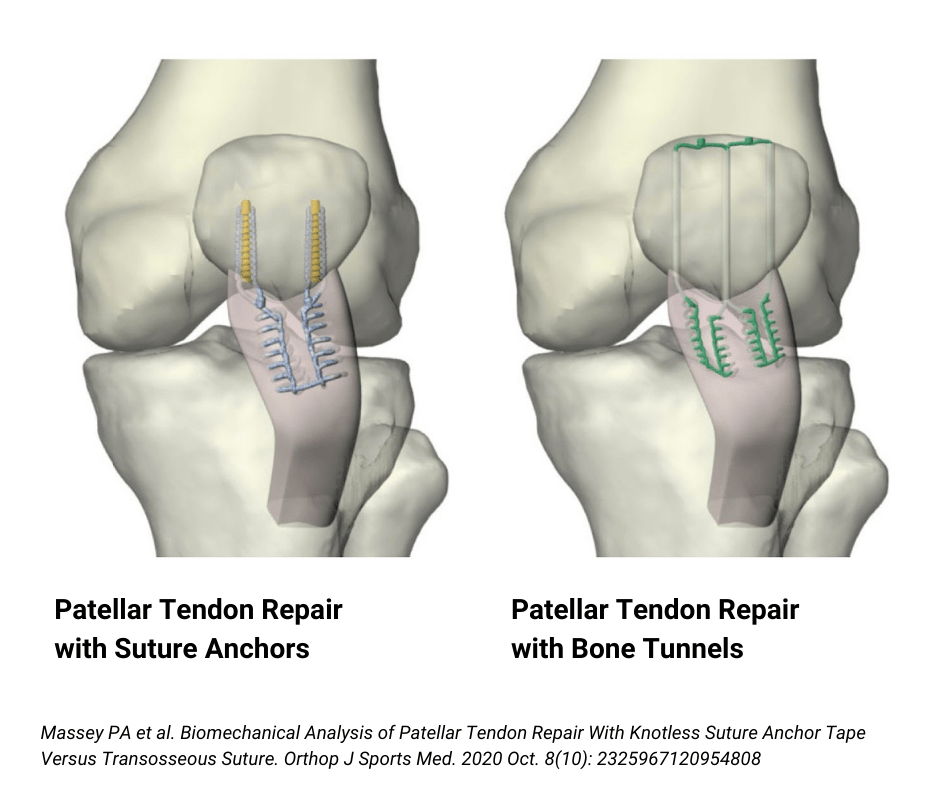
Complete patellar tendon ruptures require surgical treatment. Patellar tendon repair is performed by suturing the torn tendon and securing it back to the patella with either bone tunnels or suture anchors. This procedure is typically performed in an outpatient setting under regional anesthesia, allowing patients to return home the same day.