Many PLC injuries occur in the setting of another ligament injury, such as an ACL tear. Therefore, if an isolated ACL reconstruction is performed, and the PLC is left untreated, this can lead to early failure of the reconstructed ACL.
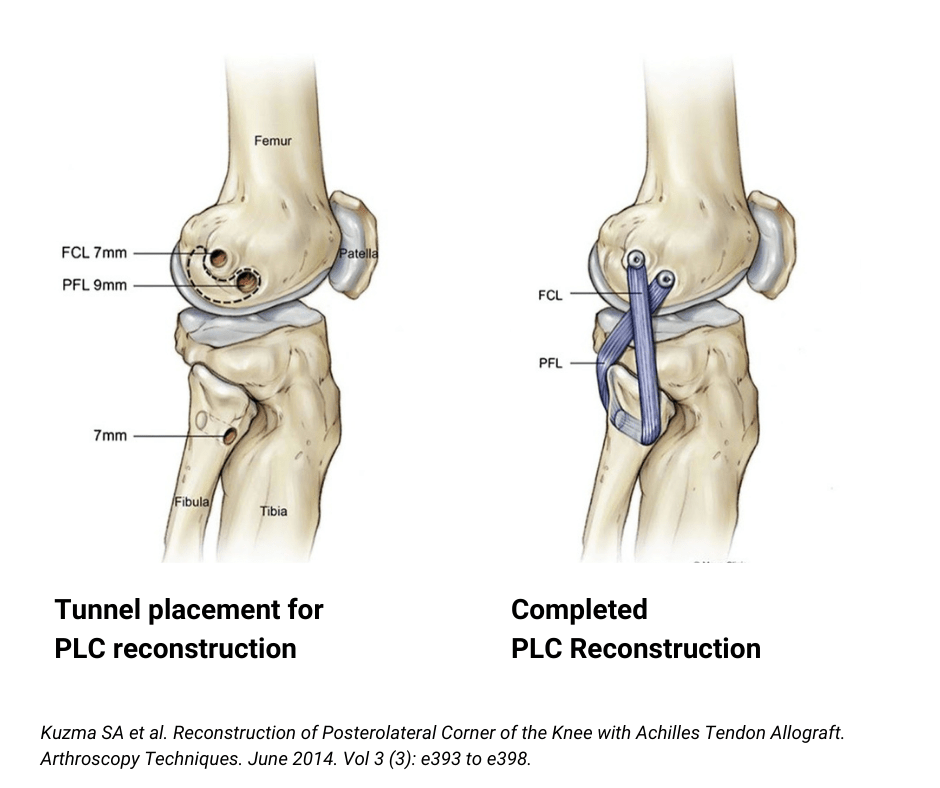
Posterolateral corner reconstruction involves placing a new ligament (graft) into the knee, which, over time, matures into the new static stabilizer of the lateral knee. This is typically done in an outpatient setting under regional anesthesia, allowing patients to return home the same day.