Conservative treatment of pectoralis major tendons is recommended in partial tendon tears, muscle belly tears, or in elderly patients. Such treatments include rest, ice, anti-inflammatories, and physical therapy.
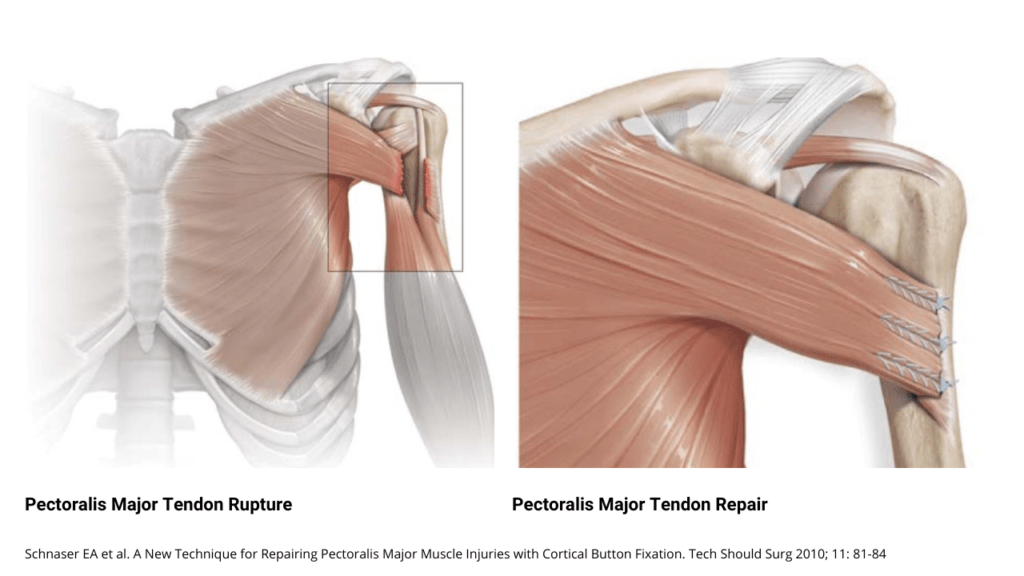
In athletes with complete ruptures who wish to regain their strength and return to their sport, operative treatment of pectoralis major is recommended. Surgical repair involves reattaching the tendon to the bone using either suture anchors or titanium buttons. This is typically done in an outpatient setting, allowing patients to return home the same day. Studies have demonstrated improved strength and function following surgical repair as compared with nonoperative treatment. In conjunction with supervised physical therapy, surgery has been shown to successfully repair the pectoralis major tendon, eliminate the deformity, improve strength, and allow patients to return to their sport.