What is it?
The acromioclavicular (AC) joint connects the collarbone (clavicle) to the acromion (the lateral end of the scapula). The AC joint is stabilized by two primary structures: 1) The AC ligament and capsule, which promotes horizontal stability of the AC joint and 2) the coraco-clavicular (C-C) ligaments, which holds down the clavicle and confers vertical stability. AC joint injuries result from a direct blow to the area and are commonly seen in contact sports, such as football and hockey, and in cyclists, who may fall over their handlebars.
WHAT ARE SIGNS AND SYMPTOMS OF AC SEPARATION?
Common symptoms of AC joint separation include:
• Pain along the AC joint
• Pain and fatigue with overhead activities
• Deformity along the AC joint
• Clicking and grinding at the AC joint
Diagnosis
In the office, a complete history and physical exam is obtained. The AC joint is examined for any deformity and tenderness to palpation. Careful evaluation of range of motion and strength are recorded. Oftentimes, specific X-Rays of both the injured and uninjured AC joints are necessary to make the diagnosis.
Treatment
Conservative treatment of AC joint separation is generally recommended in partial tears and in chronic situations. Such treatments include rest, ice, anti-inflammatories, and physical therapy. Occasionally, a cortisone injection may be recommended to reduce the pain and inflammation in the shoulder.
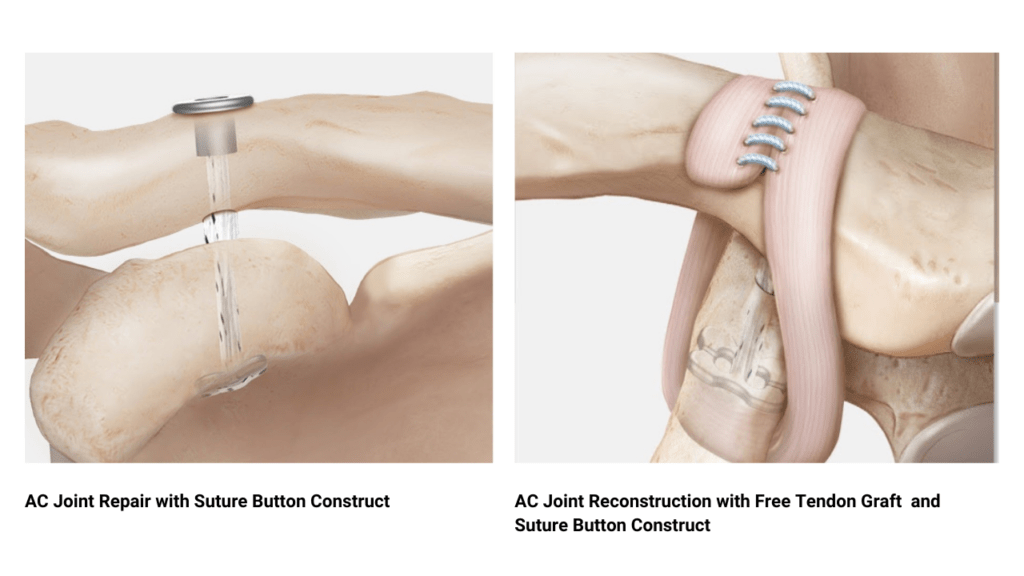
Surgical treatment of AC joint separation is recommended in severe cases (where the collarbone tents the skin) or in cases where conservative treatment has failed. AC joint repair and reconstruction aims to stabilize the joint by rebuilding the coraco-clavicular (CC) ligaments, utilizing a free tendon graft and a suture-button construct. This is typically done in an outpatient setting under regional anesthesia, allowing patients to return home the same day. In conjunction with supervised physical therapy, AC joint reconstruction has been shown to successfully stabilize the AC joint, eliminate the deformity and allow patients to return to their sport.
RECOVERY
Following surgery, patients are immobilized in a sling for six weeks (including sleep for six weeks). Physical therapy begins around three weeks after surgery. Range of motion is then initiated at six weeks, followed by strengthening at 12 weeks. Most patients can expect to return to most activities at about six months postoperatively.
AC JOINT REPAIR
The following animation demonstrates a typical repair of the AC joint. A small drill hole is placed into the clavicle and the coracoid process. A suture button is then secured underneath the coracoid, with the sutures from the button passed through the drill holes of both bones. The sutures are fed through another button, which is placed on top of the clavicle. The clavicle is then pushed down to the desired level, and the sutures are then tied over the button, completing the AC joint repair. Oftentimes, the repair is augmented by adding a free tendon graft (AC joint reconstruction), which wraps around the coracoid and clavicle to act as a “biologic suture” (not seen in animation).